

History We Can't Overlook Anymore: Details Before the Anti-Depressant Era


Photo by Towfiqu barbhuiya on Unsplash
In what follows, some of the details of history associated with both pre and posts anti-depressant eras are reviewed, drawing on Robert Whitaker's extensive reviews in this area. Much of what follows is drawn from Bob's written and verbal presentations, and provided here in summary form for easy access. I credit him for the graphics, statistics and explanations that follow. [To review more, I highly encourage you to access Bob's books and many presentations].
Depression in the Pre-Antidepressant Era. As one final set of evidence, it’s important to remember that it didn’t always used to be this way. Historical reviews show that depression was primarily a disorder of middle-aged and older persons. In 1956, 90% of first admissions to public and private hospitals in the United States for depression were 35 years and older. [See video excerpt below where Robert Whitaker walks you through some of this history: History Pre & Post Antidepressants]
In the 1930s and 1940s, fewer than one in a thousand adults in the U.S. suffered an episode of clinical depression each year. In 1955, there were only 7,250 “first admissions” for depression in state and county mental hospitals in the U.S. The total number of depressed patients in the nation’s mental hospitals that year was 38,200.
Expectations for short-term outcomes were positive, as reflected by statements from these mental health leaders at the time.
Jonathan Cole, NIMH, 1964: “Depression is, on the whole, one of the psychiatric conditions with the best prognosis for eventual recovery with or without treatment. Most depressions are self-limited.”
Nathan Kline, Journal of the American Medical Association, 1964: “In the treatment of depression, one always has an ally the fact that most depressions terminate in spontaneous remissions. This means that in many cases regardless of what one does the patient eventually will begin to get better.”
Dean Schuyler, head of the depression section at the NIMH, 1974: Most depressive episodes “will run their course and terminate with virtually complete recovery without specific intervention.”
Prognoses for long-term outcomes were also positive, as reflected by research findings from these mental health leaders:
Emil Kraepelin, 1921: Sixty percent of 450 patients hospitalized for an initial bout of depression experienced but a single bout of the illness, and only 13% had three or more episodes in their lives.
Horatio Pollock, New York State, 1931: In a long-term study of 2700 first-episode depressed patients, more than half never had another bout of depression, and only 13% had three or more episodes.
Gunnar Lundquist, Sweden, 1945: In an 18-year study of 216 patients, 49% had only a single episode, and another 21% had only one other episode.
Overall, most of those affected by depression during this period could expect to recover from a depressive episode within 12 months (80% or so), and over the long-term, depression ran an episodic course. Half of first episode patients would never experience another episode severe enough to require rehospitalization, and only 20% or so would become chronically ill.
As reflected here, depression was fundamentally understood to be an episodic disorder. Thus George Winokur, at Washington University, wrote in 1969, “Assurance can be given to a patient and to his family that subsequent episodes of illness after a first mania or even a first depression will not tend toward a more chronic course.”[1]
During this period, the prevalence of bipolar disorder ranged from one in 3000 to one in 10,000. George Winokur thus noted that there is “no basis to consider that manic depressive psychosis permanently affected those who suffered from it. In this way, it is of course different from schizophrenia.” While some people suffered multiple episodes, each episode was usually only a “few months in duration” and “in a significant number of patients, only one episode of illness occurs.” Once patients recovered, they usually had “no difficulty resuming their usual occupations” (1969 Manic Depressive Illness).
The following graphs visually represent positive outcomes for bipolar disorder in the pre-Lithium era:

The Chronicity Problem Appears: Clinical Perceptions in Early Years of Antidepressant Use. Once psychiatrists began treating their depressed patients with antidepressants, at least a few observed that these patients, once they got better and stopped taking the drugs, regularly became depressed again. While the drugs might help people over the short-term, they were putting them onto a more chronic long-term path. This was reflected in comments as early as the late 1960’s and early 1970’s:
P. Hoheisel, German physician, 1966: Exposure to antidepressants appeared to be “shortening the intervals” between depressive episodes.
Nikola Schipkowensky, Bulgarian psychiatrist, 1970: The antidepressants were inducing “a change to a more chronic course.”
There were also early concerns that antidepressants were increasing the risk that a unipolar patient would convert to a bipolar diagnosis:
1956: First case report of antidepressant-induce mania is published
1985: Swiss investigators tracking change in the patient mix at Burgholzli psychiatric hospital report that the percentage with manic symptoms jumped dramatically following the introduction of antidepressants. “Bipolar disorders increased; more patients were admitted with frequent episodes.”
1993: An American Psychiatric Association guide to depression warns: “All antidepressant treatments, including ECT, may provoke manic or hypomanic episodes.”
Yale investigators went on to quantify the risk of Conversion to a bipolar diagnosis with antidepressant use [A. Martin. “Age effects on antidepressant-induced manic conversion,” Arch of Pediatrics & Adolescent Medicine(2002) 158: 773-80]. They analyzed the records of 87,920 patients, ages 0 to 29, initially diagnosed with an anxiety or non bipolar mood disorder from 1997-2001. The median follow-up time was 41 weeks. They reported on the number of patients who converted to a bipolar diagnosis according to whether they were exposed to an antidepressant:

In a survey of members of the Depressive and Manic-Depressive Association, 60 percent of those with a bipolar diagnosis had initially fallen ill with major depression and had turned bipolar after exposure to an antidepressant. [R. El-Mallakh. “Use of antidepressants to treat depression in bipolar disorder.” Psychiatric Services 53 (2002): 58-84].
Fred Goodwin, former director of the National Institute of Mental Health, 2005: “If you create iatrogenically a bipolar patient, that patient is likely to have recurrences of bipolar illness even if the offending antidepressant is discontinued. The evidence shows that once a patient has had a manic episode, he or she is more likely to have another one, even without the antidepressant stimulation.”
An Episodic Illness Turns Chronic in the Antidepressant Era. By the 1980’s and especially in the 1990’s and beyond, this new observation of chronicity in depression became accepted as a more truthful understanding of the inherent nature of clinical depression as a whole:
National Institute of Mental Health Panel on mood disorders, 1985: “Improved approaches to the description and classification of [mood] disorders and new epidemiologic studies [have] demonstrated the recurrent and chronic nature of these illnesses, and the extent to which they represent a continual source of distress and dysfunction for affected individuals.”
The APA Acknowledges Change in Course of Depression in Modern Era American Psychiatric Association’s Textbook of Psychiatry, 1999: It used to be believed that “most patients would eventually recover from a major depressive episode. However, more extensive studies have disproved this assumption.” It was now known that “depression is a highly recurrent and pernicious disorder.”
Rather than confront the possibility that antidepressants were making patients chronically ill, psychiatry–as a field–told a new story about the course of unmedicated depression. Early epidemiological studies showing that patients regularly recovered from a depressive episode and often stayed well must have been “wrong,” they said. Modern research had shown that depression was a chronic illness, which required continual medication. And indeed, studies now showed that patients treated with antidepressants fared quite poorly over the long term, even though they were maintained on the drugs. (The poor outcomes were blamed on the disease, not the drug, however.)
Prior to the widespread use of antidepressants, depressed patients regularly got well, and many never suffered a second bout of major depression. Today, the overwhelming majority of patients diagnosed with major depression and treated with antidepressants suffer recurrent bouts of the illness, as evidenced by studies such as these:
Does incomplete recovery from first lifetime major depressive episode herald a chronic course of illness? Judd, L. American Journal of Psychiatry 157 (2000):1501-4. Two-thirds of all unipolar depressed patients either do not respond to initial treatment with an antidepressant or only partially respond, and these patients fare poorly over the long-term. NIMH-funded investigators reported in this study that “resolution of major depressive episode with residual subthreshold depressive symptoms, even the first lifetime episode, appears to be the first step of a more severe, relapsing, and chronic future course.”
One-year clinical outcomes of depressed public sector outpatients. Rush, J. Biological Psychiatry 56 (2004):46-53. Psychiatrists at Texas Southwestern Medical Center in Dallas noted that most clinical studies “cherry-pick” patients most likely to respond well to an antidepressant. In this long-term study of “real-world” patients, only about 13% of the patients stayed better for any length of time. These “findings reveal remarkably low response and remission rates,” the investigators concluded.
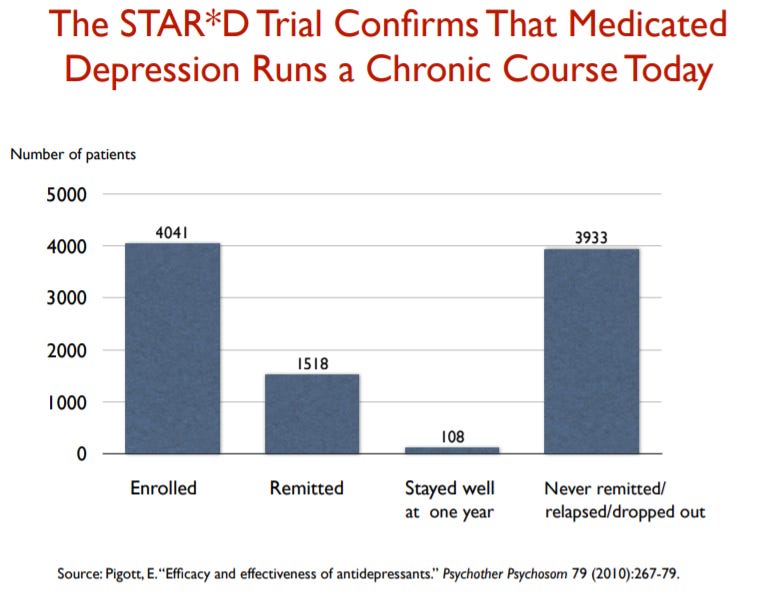
Efficacy and Effectiveness of Antidepressants. Pigott, H. Psychotherapy and Psychosomatics, 79 (2010), 267-279. In a large NIMH trial of 4,041 “real-world” outpatients, only 108 patients remitted and stayed well and in the trial during the one-year follow-up.
Modern Course of Bipolar Illness: Worsening Long-term Course in Drug Era. Anthansious Koukoulos wrote in 1983, “The general impression of clinicians today is that the course of recurrences of manic-depressive illness has substantially changed in the last 20 years. The recurrences of many patients have become more frequent. One sees more manias and hypomanias . . . more rapid cyclers and more chronic depressions.”
Compared to the prevalence reported earlier, one in 50 adults now reports experiencing bipolar disorder. The changes now include the following:
More recurrent episodes and more rapid cycling
Low-level depression between episodes
Only 33% enjoy good functional outcomes (compared to 70% to 85% in pre-drug era)
Long-term cognitive impairment (which wasn’t seen in pre-drug era)
Physical problems related to long-term medication use
Risk of early death

Lewis Judd wrote in 2008, “It is now well established that bipolar disorders are chronic, with a course characterized by frequent affective episode recurrence.”
Experts Recognize the Decline in Bipolar Outcomes:
Carlos Zarate, head of NIMH Mood Disorders Program, 2000: “In the era prior to pharmacotherapy, poor outcome in mania was considered a relatively rare occurrence. However, modern outcome studies have found that a majority of bipolar patients evidence high rates of functional impairment.”
Ross Baldessarini, Harvard Medical School, 2007. “Prognosis for bipolar disorder was once considered relatively favorable, but contemporary findings suggest that disability and poor outcomes are prevalent, despite major therapeutic advances.”
Fred Goodwin, 2008 “The illness has been altered. Today we have a lot more rapid cycling than we described in the first edition [of his book, Manic Depressive Illness], a lot more mixed states than we described in the first edition, a lot more lithium resistance, and a lot more lithium treatment failure than we described in the first edition. The illness is not what Kraepelin described any more.”
The Burden of Bipolar Illness on Society Today:
In 1955, there were 12,750 adults hospitalized with bipolar illness in the United States. Today there are nearly six million adults in the United States with this diagnosis.
According to the Johns Hopkins School of Public Health, 83 percent of people diagnosed with bipolar are “severely impaired” in some facet of their lives. (5 million adults.)
Bipolar illness is now said to be the sixth leading cause of medical-related disability in the world.
We end with a more optimistic and reassuring glimpse from history, reflecting the kind of heartening history that exists around other, more gentle and relationship-oriented approaches to caring for those facing serious mental and emotional challenges: A Historical Example of Sustainable Healing.
Notes:
[1] Manic Depressive Illness