

7 take-away messages from the recent Washington, D.C. summit on safe tapering from psychiatric medication
65 million Americans are currently taking a psychiatric medication. How many of them, their family, and their doctors understand how to safely taper if they ever want to come off the drug?


Cameron LaBar was 9-years-old when he was diagnosed by a New Jersey doctor with anxiety and OCD, and started on Paxil. For the next two decades of his life, continued, evolving medical treatment became an unquestioned feature of his life.
“I was always told that I had a chemical imbalance and that this was treating that,” he shared at last Monday’s “Mental Health and Overmedicalization Summit” in Washington, D.C. He heard this explanation from his doctor. And he heard it from his parents and other family members through much of his childhood. “I believed that I needed this and that I was treating something very targeted to help me to function.”
“I was never approached or never ever had a discussion about an off-ramp or (eventually) reducing these medications,” he added. Every night he would take them, he remembers. “But there was never a discussion of when is the finish line, you know, when am I done taking this? That discussion never happened.”
Cameron wishes it had.
‘Wait, so maybe this isn’t really who I am?’
At the time he was first diagnosed and prescribed medication, Cameron’s family had just moved to a new state and his father was working nearly 80 hours a week, leaving his mother to handle this scared 9-year-old boy and his four siblings. Reflecting back on the moment he began to feel paralyzed by fear as a child, Cameron talks today about the limitations in this early deliberation:
“I just don’t think there was enough conversation …to ask the questions of: What does his sleep look like? Is he sharing a room with a sibling who gets up way earlier than he does? What is his diet like? Did he just move somewhere to another state where he’s not outside and playing and in the sun as much as he used to be?”
“All of these different types of questions I don’t think were ever asked and it was just kind of like a very quick labeling from the neurologist that I had a problem and it was a chemical imbalance and it needed to be fixed.”
For the subsequent 26 years, Cameron has been on medication. After being treated for most of his life, Cameron reflected, “it took a really long time for me to realize that the things that I thought were character traits about me being tired, drowsy, forgetful, numb, indifferent to going out and doing things or to having friends or to starting a relationship—it took a really long time for me to end up figuring out that those weren’t character traits. Those weren’t parts of my personality … Those were side effects of a medication.”
This clash in interpretations is central to Cameron’s story. Two other examples of this:
Cameron recalled a panic attack at a summer camp where he wasn’t getting enough sleep and consuming too much caffeine. When the doctor found out what happened, he left with another prescription—a Benzo. “There was no discussion of ‘Well, what happened at the summer camp?” (Moderator Kim Witczak interjected saying “this is very, very common where people go in with the side effects and they end up with another and it could be the drug side effect and they end up going out with another you know as you said another prescription.”).
Cameron described previously trying to go off medication—and being told by the doctor to cut the dosage in half. This sudden and dramatic reduction, he said, “would throw me into such a severe panic and response and I would immediately go back up on the dose.” The doctor would subsequently reaffirm to him that these scary experiences, rather than a withdrawal effect, was “a part of your underlying condition and that you probably need the medication.” (Countering this automatic labeling of withdrawal effects as a “return of the depression” has been a core message of Peter Breggin and other authors over the last several decades).
Can you tell the difference between effects from depression and antidepressants?

Dear readers — this is one of the most important things I’ve ever published. With roots that date back to my 2006-2009 University of Illinois dissertation on depression treatment, I’ve been thinking about this question for two decades now.
Cameron eventually stumbled on videos from British researcher Mark Horowitz, one of the leading experts in tapering off of antidepressants, which he said, “helped me to understand that side effects are so common and that this isn’t, you know, it’s not a part of who you are necessarily.”
This realization prompted this man to initiate a measured, careful, gentle tapering process three years ago. Now 35, Cameron describes feeling better than he has in a long time—and on a lower dose than he has in a long time. “I’m down to about 7 and 12 milligrams of Lexapro.”
Cameron describes recently getting through a “really hard part of withdrawal” and now taking a break at his current dosage. “It’s probably going to take me another three, four or five years to get the rest of the way just given how these drugs work.”
Cameron had become accustomed to these many side effects—and the idea that they were not “some underlying part of who I am” has changed so much.
“It took me 20 years to find that out,” Cameron said. He admitted some deep frustration with that realization, as he continues to taper. “So trying to deal with that….I could have figured this out a lot sooner, right?”
“The way I’m functioning now, I could have functioned as a human being all along, right? I could have had friendships and I could have not been numb and I could have formed (romantic) relationships.
“I’ve missed a lot of life and a lot of my experience … I never got to experience the full range of emotions and feeling of being human. And that’s been really, really hard.”

(This is a screenshot. Watch the full talk on Cameron’s Instagram here)
Cameron was one of several patients who spoke at the summit, hosted by the MAHA Institute—along with researchers and other experts. Two of my own dear friends and colleagues spoke, from my two decades of interest in this topic since my dissertation on antidepressants.
I’d like to highlight ten other moments from the day-long conference worthy of attention. But not before highlighting two important qualifiers shared by Cooper Davis, the executive director of Intercompass Initiative—a nonprofit organization that helps people make more informed choices about taking and safely tapering off psychiatric drugs:
Not “anti-medication.” “I want to be clear, we are not anti-medication. We are just committed to true informed choice. And those things should not be confused. And we believe true informed choice is in fact a human right.” He makes clear the summit’s stated frame is not “no one should take medication,” but that when a medication isn’t working or people don’t want to be taking it anymore, they deserve a safer process to taper off.
Don’t ignore stories. “Too often when people speak about them, their stories are dismissed as merely anecdotal or unfortunate,” Cooper added. “But anecdotes are in fact evidence. Subjective experience matters.” Another speaker, Kim Witczak, likewise said, “These are not anecdotes. These are real lives.”
In what follows I recap 7 other highlight talks from the conference, taking the time to give the full context of why they matter. While this won’t be of interest to everyone, it will be important to a subset of people who have lived it. So I’ve chosen to go deep here, giving those readers the details they’ll want. You can click below to see the entire transcript—and here and here to watch the entire conference.

Note: None of this substitutes for medical advice. And it’s always advisable to make adjustments to medication with medical guidance and support. But it’s crucial to remember changes need to happen gradually—not sudden and dramatic.
1. ‘I was a child and I didn’t have the words to explain what was happening’ (and the dangers of fast tapering). Danielle’s story
Danielle Gansky was prescribed psychiatric medication at 7 years old. “I was far too young to understand what they were, let alone the lasting impact they would have on my developing brain,” she said. But in the second grade, a teacher noticed she was fidgety, distracted, and not fully keeping up academically—advising her parents to see a psychiatrist for an ADHD evaluation.
“I was quickly diagnosed, labeled, and medicated,” she said, recalling they told her she had a learning disability too. About her experience being prescribed ADHD stimulants like Adderall and Ritalin, she said, “I still remember how agitated and moody they made me feel. This was completely out of character for me as I was a happy, sweet, silly kid.”
“Adverse side effects were interpreted as new diagnoses and more drugs were prescribed to treat the problems that the medications themselves had caused. This spiraled into a prescription cascade of antidepressants, benzodiazepines, mood stabilizers, and antipsychotics all before my 10th birthday.”
“None of it ever felt right. But I was a child and I didn’t have the words to explain what was happening. And I didn’t have the authority to challenge it.
Throughout my teens, every drug-induced effect that made me feel terrible was blamed on my so-called underlying disorder.
As I got older, I found online forums of people describing their harms from antidepressants and began to realize the drugs might be the problem. But when she brought her concerns to a doctor and asked if the medications could be making her feel worse, the doctor insisted that wasn’t possible—and that, instead, this meant her OCD and anxiety were “getting worse” and that she “needed higher doses of the SSRI to treat it effectively.”
After college, at age 23 years old, she said “I wanted to see who I was underneath the chemicals.”
“Although I had been on antidepressants my whole life, all while my brain was literally developing, my doctor tapered me off in just 6 weeks,” she said, “which was far too fast.”
(She adds, “But my doctor wasn’t acting recklessly. He was following the standard medical guidance doctors are taught to use”).
What followed the rapid taper, she said, “was a severe full body neurological crisis, a non-stop living nightmare of physical and psychological torment and suffering I didn’t know was humanly possible. My brain felt like it was on fire. Waves of visceral terror and violent inner agitation ripped through me. I was crawling out of my skin for hours each day. I rocked back and forth in the fetal position on the floor, screaming in excruciating pain. Rage surged through me that was completely out of character as I’ve never (experienced) this type of anger.”
“I was always gentle and kind,” she added, but this rapid and dramatic taper “brought out a violence in me that never existed. My brain and body were malfunctioning, feeling like I was being poisoned. It was an attack on my nervous system. Simply being alive felt unbearable.”
When Danielle went back to her doctor and told him she was in withdrawal, she was told “antidepressant withdrawal doesn’t exist, that the medication was out of my system, and my symptoms were proof I needed the medication.”
“His credentials and expertise automatically outweighed my lived experience,” she now recalls, “and the very injury caused by the drugs was used to justify putting me back on them.”
After months of suffering, she recalls feeling she “had no choice but to reinstate the antidepressant even though I felt as though it was poisoning me.” But these neurological effects didn’t go away after re-instituting the medication and she’s experienced them for 7 years now—leading her to believe she had experienced a more of a “lasting injury to my brain and nervous system” caused, she believes, from the fast pace of tapering directed by her doctor.
And, of course, the original decision to put her on. Looking back now, she says “My completely normal childhood behavior was pathologized. I wasn’t in crisis. I wasn’t struggling or acting out. I was simply a fidgety, shy, sensitive little girl who didn’t fit the mold of how a child was supposed to behave in a classroom setting.”
“I went from being a vibrant, joyful, happy person who loved life to being chronically ill and disabled….My creativity, my intelligence, my emotions, everything that made me me was ripped away. I was bedridden and housebound for years. My 20s were spent grieving a life that I felt was taken from me far too soon, watching everyone else move forward while I remained stuck trapped in a body that felt like a prison.”
She’s still taking the same SSRI prescribed as a child, still struggling to come off due to severe debilitating withdrawals. Danielle is now tapering extremely slowly using “hyperbolic tapering” which is the safest method known. She reduces by just one tenth of a milligram, for example 53.6 milligrams down to 53.3—which is less than 1% decreases, because that’s all her nervous system can handle. Even those tiny reductions are challenging, she said.
“What happened to me is not rare,” she said. “My story is just one window into a much larger hidden public health crisis.” Rather than mere “withdrawal,” which she suggested can be a “misnomer,” inappropriately fast withdrawal can lead to “neurological injury that can persist for years and may be permanent for some. The suffering is so immense many people end up taking their lives in withdrawal.”
“It’s my life’s mission to make sure to create changes to make sure this doesn’t happen to anyone else,” she said. “My inner reality was dismissed at every turn”—noting that the medication label doesn’t warn you people that these drugs can “fundamentally alter your brain” to such a degree that tapering off can be difficult, even impossible for some.
Neither do the labels caution enough at the “loss of emotions and the ability to feel love leaving you.” She concluded by saying, “People have a fundamental right to full and honest information about the harms of SSRIs before they ever take them. When those risks are withheld, it is not just unethical. It’s a violation of basic human rights.
Danielle called for stronger warnings to patients about the true, life-altering and sometimes permanent risk. And she called for “federally endorsed evidence-based tapering guidelines so people can come off their antidepressants safely without risking a brain injury.”
“People need to be aware this can happen to them so they can truly make informed decisions,” Danielle later said. “We need evidence-based tapering guidelines to help people safely come off these drugs,” agreed Andrea Beckel-Mitchener, Acting Director of the National Institute of Mental Health (NIMH) - emphasizing a need to “broaden the evidence base of what de-prescribing is.”
Danielle’s story is a cautionary tale about how drug-induced effects are interpreted as new diagnoses, leading to more drugs: initial struggles → diagnosis → medication → adverse effects → more diagnosis/medication. In this way, childhood behavior can become lifelong medical identity.

2. Laura Delano’s stunning message: From hopelessness to beauty
I’ve known Laura for a number of years, and wrote about her awhile back for Meridian Magazine: “Your Urge to Die, is Really an Urge to Live Differently.” Her talk at this summit was the stand-out highlight.
Explaining her decision to found Intercompass Initiative, Laura Delano said “my decision to start ICI came after I realized that my parents and I had never actually made a truly informed choice” about her 14 years of treatment. “I grew up on psychiatric drugs, accumulating an alphabet soup of diagnosis through my teens and 20s. Over those years, as I carefully complied with my treatment, my physical health, creativity, sexuality, relationships, connection to God and nature and meaning and purpose, all of it was overtaken by medicalization.”
“I became a list of symptoms to be managed,” she said. “I was in endless therapy and admitted myself to many programs and hospitals. I was on two meds, then three, then four, then five. Along the way, life fell apart.”
“At age 25, told by my psychiatrist I was so severely mentally ill that I was now resistant to all treatment, I tried to kill myself. I am far from the only one.”
“Not a day goes by that I don’t thank my lucky stars I made it through alive and that I eventually realized this medicalized understanding of myself had become a prison.” After finding a broader way to think about it, Laura says she gradually tapered off “all the meds I’d been told I’d need forever to stay alive.”
That was 16 years ago. Today, she’s leading an international non-profit with her supportive partner Cooper, and raising beautiful children. Laura then defined “medicalization” as “what happens when we take complex human struggles and call them a disease. It’s the act of pathologizing natural, understandable, even common sensible responses to our individual lives and the broader world in which we live.”
“To be clear, questioning medicalization isn’t about denying suffering or denying that many people experience real benefit from psychiatric treatments,” she said, “especially in the short term. It’s about asking what our culture has sacrificed by telling generations of Americans that being human is a disease.”
“Millions of our young people now grow up convinced something is wrong with them. They’ve been taught to take their despair and self-doubt and loneliness, their shame and obsession and alienation, their struggles in friendship and romance, their fear and angst and grief. and translate all of these experiences into symptoms of incurable brain pathology requiring lifelong pharmaceutical use.”
Many have grown convinced, as she once was, Laura said, that “their life’s main purpose is symptom management with endless pills and therapy and programs. They are convinced the only way the depth of their pain can be seen, understood, and validated is through medicalizing it. They are convinced the only people qualified to help them are those with letters after their names.”
“And when they’ve done all this and their dysfunction and disability have only worsened, they’re told this means their illness has progressed—that the reason their psychiatric treatments aren’t helping is that their brain disease is just too far gone.”
“This is a story of hopelessness. And it’s a story that I and countless others have grown up believing in deeply.”
Laura then cited philosopher and social critic Ivan Illich who warned 50 years ago of the “deep harm caused when a culture becomes overly medicalized.” What he called medical iatrogenesis occurs when health professionals inadvertently “destroy the potential of people to deal with their human weakness, vulnerability, and uniqueness in a personal and autonomous way.”
“We are now living with these consequences. Tens of millions of Americans are convinced their suffering is a sign that they are permanently broken rather than a signal about the world they’re trying to live in—a world of screens and social media, broken sleep, too much stress, too little sunlight, too little movement, too little real food, too little solitude, too little face-to-face time with others in local meaningful community.”
Laura then cited off key statistics in terms of where we are as a country with mental health:
Nearly one in four adults has a psychiatric diagnosis.
40% of high schoolers report being persistently hopeless with 9% attempting suicide.
Suicide rates have climbed sharply across nearly every age group since the late 1990s.
Nearly 50,000 Americans killed themselves in 2023, the highest number ever recorded.
At the same time, nearly 65 million Americans are taking psychiatric drugs, including around four million children.
“We’re told this is a mental health crisis. But what if this crisis is in large part fueled by misinterpretation, by medicalizing struggles that were never medical to begin with and don’t have medical solutions?”
“Just as we have woken up to the misleading story sold to us by the pain management industry that all physical pain is a problem to be eradicated with safe effective pharmaceuticals that are not dependence forming; we are now waking up to the false promises of this industry of mental health—an industry that’s taught us emotional pain is a symptom to eradicate with safe, effective pharmaceuticals you’ll likely need for life. But if not, don’t worry. You can easily stop.
Laura’s talk was a challenge to this narrative she and other participants see as “deceptive.”
“For a long time, it’s been mostly patients sounding the alarm on overmedicalization—people who have lived its consequences firsthand, realized there was in fact a future beyond chronic illness and had no choice but to develop safe psychiatric medication tapering protocols because their doctors couldn’t or wouldn’t help them.”
“Prescribers are trained to put people on psychiatric medications, not help them safely taper off. They aren’t taught about the dependence forming nature of all psychiatric medications (not just benzodiazepines), or that the difficulties patients face when stopping their medications may well be withdrawal, not relapse.
They don’t realize that tapering slowly doesn’t mean over days, weeks, or months, but possibly over years. Patients had no choice but to develop some of the world’s most careful tapering protocols for themselves and build online communities to share them freely with one another because there was nowhere else to turn for reliable information.
(Check out Laura’s excellent 2025 book here).
Thank goodness this is now changing. Prescribers and mental health professionals are realizing that they, like us patients, have been misled by the quick fix promises of the industry they work in. They came to this work because they wanted to help suffering people and were not given the information they needed.
This is an information problem we are all in together. There are many out there who want to keep us divided. They want to polarize and politicize this conversation, making it about right versus left, patient versus doctor, us versus them, quackery versus science, pro- versus anti-medication.
We mustn’t let them. This should not be a war zone. This should be a community table where we come together to learn from one another and embrace vulnerability, humility, and curiosity. Working together to once and for all address this national crisis. We owe it to the 65 million Americans on these medications to build safe off-ramps that should have been provided all along for those who want or need them.
And we owe it to our children who hold the future of this country in their sweet, sensitive, impressionable hearts to remember what it means to be human. That emotional pain is part of being alive. That meaningful help comes in countless forms beyond a pill bottle. Only then will the world they’ve inherited begin to make sense again.
Based on Laura’s other comments at the summit, we might ask ourselves: Of the roughly 65 million Americans currently on psychiatric meds, how many of them have been meaningfully informed about how to come off safely at the end of that journey if they decide they don’t want to take them anymore?
3. Lauren Friedman’s pain of struggling to feel deeply and connect intimately
Lauren Friedman described living with a condition called post-SSRI sexual dysfunction. 50 to 70% of all patients taking these antidepressants will have sexual side effects—with these potentially enduring after treatment ends. What patients are not warned about is that these side effects can be permanent long after you stop the last drug dose. Um, and PSSD is not just low libido. It is a full nervous system injury in which you lose total sexual function neurologically through essentially nervous system damage. So, the hallmark symptom of PSSD is genital numbness. Yes. like complete loss of sensation in your genitals.
“I clearly hate to talk about this, but my clitoris is completely numb as if it’s the back of my elbow. I have no sensation internally. I’m 23 years old.”
Some lose the ability to orgasm, with no libido—which some experience, Lauren said, like “a sudden onset chemical asexuality.”
There can be a loss of emotional function as well—something Lauren has experienced. “Before this, I was a super emotional empathetic, loving, caring, like Sylvia Plath reading and resonating girl.”
But the day she woke up to this injury, she felt a profound shift internally in her ability to feel—something that has lasted for years. “To this day, I can’t feel love for my own mother, which is the hardest thing on earth. I can’t feel connection or love for my friends, or even pleasure in music (though I had been) a songwriter since I was a child. It was my outlet.”
Lauren calls the many kinds of love experienced in “central, intoxicating, worthwhile, and fulfilling parts of the human experience. These aren’t luxuries. And to remove someone’s ability to participate not just physically through sex … but to remove someone’s ability to emotionally connect with another human being is a crime.”
This grieving young woman then went on to allege that Eli Lilly, the maker of Prozac, withheld for too long their full knowledge of the likelihood of these kinds of effects. (The current FDA Prozac labeling does acknowledge that “symptoms of sexual dysfunction occasionally persist after discontinuation of fluoxetine treatment”—adding that estimates of SSRI sexual side effects in labeling are “likely to underestimate their actual incidence.” This warning language was added in 2011, 23 years after the medication’s release in 1988. Advocacy groups such as the PSSD Network point to Eli Lilly/FDA from 2011 as evidence that the company was aware of persistent sexual dysfunction reports years earlier).
Since this specific diagnosis hasn’t been called out on the label, Lauren said, “I quite literally had no way of knowing that this was possible or that this could happen to me.”
“Had I known that this medication had the capacity to cause permanent loss of sexual and emotional function, I would have sought after alternatives….But that decision was made for me.”
Throughout Lauren’s story, her grief and indignation are apparent—even if her words remain calm. She calls her condition “torturous,” “horrific” and “inhumane suffering” with “these things that are so central (to life are) able to be removed” (she also uses a heartbreaking language of being “sexually defunct and emotionally lobotomized”).
At one point, she alleges that “life is not worth living when you can’t feel it or participate in it”—which this author points out would be a dangerous idea to entertain for anyone experiencing one of many reasons why they aren’t feeling as much as they used to. Better to remember that things can still change and improve—and in the meanwhile, there are still important things to learn, experience and offer to the world.
Lauren frequently speaks of her condition as permanent and lifelong, but acknowledges at the end, “there is evidence that this may be reversible with intervention.”
“We’ve been blindsided, betrayed, and maimed by the industry that we were told and instructed to trust, and we trusted fully given we took these medications, and now we’ve been offered no way back to our lives or humanities.”
I feel so deeply humiliated and dehumanized to share to a group of strangers in the press and inevitably the internet…. I’m a senior in College of Vanderbilt. I go back in the fall. I’d rather my peers not know this about me because this is what the situation requires.”
“I’m here to ….show that these medications are far from benign. People deserve to know the truth.
Lauren’s testimony is intense, but the policy message is simple: people cannot give informed consent if a serious potential outcome is absent from labels and clinical conversations.
Admiral Brian Christine reiterated in another presentation, “The decision to prescribe SSRIs should always… come with a full understanding of both the benefits and the risk.”
“Many veterans don’t understand what they’re getting into,” said Derek Blumke about many vets being treated. “Their families don’t understand what they’re getting into.”
4. What does safe tapering actually look like (why linear tapering is a big mistake), by expert Mark Horwitz
Mark Horowitz is an associate professor of psychiatry who works in Australia and the UK and had his own experience coming off the medications. He began his presentation saying, “Many people have tried multiple times to stop um psychiatric drugs and very much want to get off them. Not everybody, but many. And the question is why do so many people find it difficult to stop?”
“The answer is not a lack of motivation or psychological dependence as some people suggest. The reason is that the way we currently stop these drugs is biologically mismatched to how they work.”
The researcher went on to explain that, contrary to what many people assume, there is not a straight line relationship between dosage and effects on the brain. “If you double the dose from 20 mg to 40 mg, it doesn’t increase the effect on the brain very much at all”—with even a tiny dose of 2 milligrams having about half the effect of 40 milligram.
He compares this psychopharmaceutical principle to a “game of musical chairs. It’s easier to find a spot at the beginning of the game. As there’s more and more drugs in the system, the receptors fill up, it becomes harder to find a spot, and you get diminishing returns.
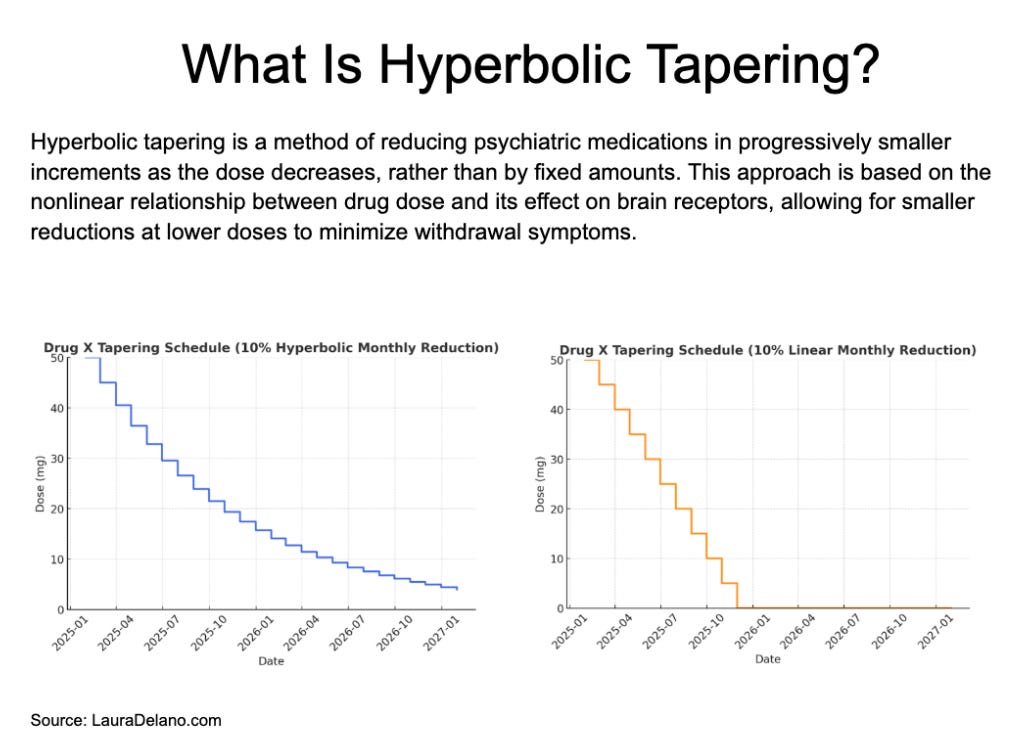
This is the problem with a typical linear tapering plan often recommended by doctors and most guidelines: “you start off at 20 milligrams, go down to 15, 10, 5, 0.”
Although this looks gradual on paper, the first reduction from 20 to 15 is on the level of the brain, a “tiny little reduction.” Although the next reduction (15 to 10) looks equal, it’s actually twice as large in its physiological effect—with the third reduction (10 to 5) twice as large again.
The last reduction, from 5 mg to 0 milligrams, then becomes the hardest of all. He summarized, “So what looks like a gentle taper actually involves jumping off a cliff at the end.”
This corresponds to patient experience, where Horowitz says “the beginning of the taper is fairly easy or easier and they and they struggle most at the end.”
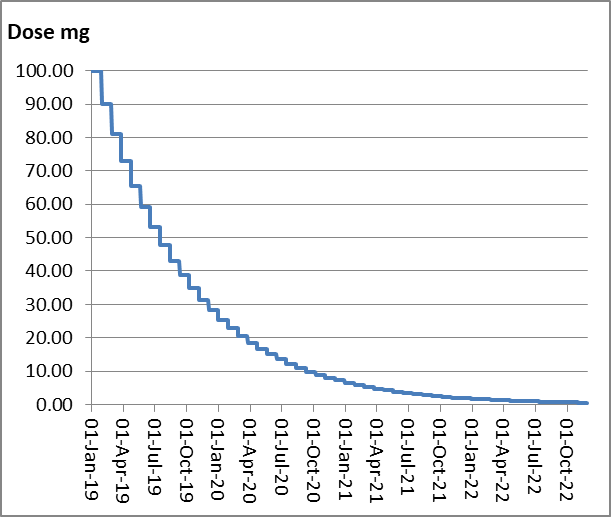
Here’s the alternative: “Instead of reducing by a fixed amount of dose, you reduce so that each step produces a similar change in the brain. And this requires smaller and smaller dose reductions. So that the final reductions are very tiny doses, much smaller than the currently available tablets or capsules, so that you’re not jumping off that cliff. You’re walking down it step by step.”
The name of this wiser, safer tapering approach is “hyperbolic tapering” because it follows the hyperbola of the graph as if you’re walking down the curve, he explains.
(I like to compare this to flying a plane—where you drop more quickly at first, and have to slowly edge into the last moments).
A good rule of thumb is to reduce by about 10% of your most recent dose each month, he explained—so the amount of decrease “gets smaller and smaller.”
This needs to be individualized, however, and adjusted depending on how people respond. “Some people can go faster, some people need to go slower. There are some recognized risk factors but the speed needs to be adjusted to the individual based on careful monitoring.”
That means holding, pausing or adjusting the taper if symptoms become difficult.
Importantly, Horowitz pointed out, the smallest dose available in most antidepressants still has about 80% of the effect of the drug’s maximum licensed dose. That explains why it’s not a good idea to just stop for good after getting to the smallest tablet. “People are often told you’re just on a small dose, you can stop it. And that’s never the case. You know, your body doesn’t know that you’re putting a small tablet in your mouth. It only cares about the effect on receptors.”
That’s a trap that people get caught in. But the good news is in a study of 900 patients who had almost all been unable to stop their drugs with the traditional taper recommended by their doctors, almost three-quarters could stop with this gradual hyperbolic approach to coming off their drugs. They experienced fewer withdrawal effects—and many could have even had better success, he believes with even slower tapers.
Why don’t more people understand this? Four reasons:
“Most clinicians are not trained to recognize withdrawal or to take medications in this way. As a result, withdrawal symptoms are often misinterpreted as relapse and treatment is continued unnecessarily.”
“Many clinicians are not accustomed to prescribing liquids or compounded medications required for this technique.” He explained it’s not possible to implement this approach well only with tablets.
“Most psychiatric drugs in the US are available as liquids or can be made up with smaller doses by compounding pharmacies”—noting that it “would be useful if the FDA were to mandate liquids or small dose tablets for all psychiatric drugs in the same way as car manufacturers mandate braks on cars.”
“Existing guidelines often only tepidly acknowledge withdrawal and do not provide practical detail. Clinicians are left without specific tapering schedules or strategies for managing symptoms. This is true of the recent American Society of Clinical Psychology guidance which avoids these major issues and offers no practical help for clinicians on the ground. This is what we tried to solve with the Maudsley deprescribing guidelines which offers advice to clinicians.”
Horowitz shared a few additional notes, starting with a few cautions:
“Dosing less often, for example, every second day often backfires because it leads to wildly oscillating levels in the blood.”
In a New York Times story on new deprescribing guidelines of American Society of Clinical Psychopharmacology, one expert pushed back on encouragement of “slow tapering” across the board—insisting that longer half-life drugs like Prozac can “generally be stopped abruptly.” Horowitz responded to this, saying “Just because the drug leaves the system in a few weeks is not long enough to let the brain reset. And in fact, these drugs have withdrawal risks almost as high as other drugs in the same class. So there is no free ride off these drugs.” (Anders Sorensen elaborated in his remarks, noting that having a longer half-life as a drug “just means that the withdrawal reactions are delayed not that they’re absent….Yes, it’s a good thing that a drug leaves the body a bit slower because again withdrawal is the drug leaving the body faster than the body can adapt…that doesn’t mean that there are no withdrawals whatsoever….Don’t follow that advice (to quickly taper). The hyperbolic curves …are exactly the same with Prozac as in any other SSRI).”
When a medication is started, Horowitz recommended that “informed consent should include expected duration of treatment and a plan to review and potentially stop right from the beginning. Patients should not begin these drugs, assuming they are indefinite.” A treatment plan should include an end goal date—suggesting a regular six month medication review, comparing ongoing benefits vs. harm—and revisiting “a clear plan to continue or to stop.”
“Health care systems are set up to start medications quickly but they do not provide the time, support or infrastructure to help people come off them safely.”
“To summarize, withdrawal is a physiological process that can be prolonged. Current tapering methods are often biologically mismatched to how these drugs work. Safer methods already exist based on aligning dose reductions with the brain’s response, such as hyperbolic tapering.”
“Knowledge about how to recognize withdrawal, distinguish it from relapse, and safely stop psychiatric drugs needs to be embedded in medical education as much as starting the drugs are. At the moment there’s a huge hole in education and service which is seen in escalating numbers of people on these drugs who cannot get off.”
5. Understandable reactions to difficult environments or signs of illness? Nick’s story
What happens when the system treats friction with broken environments as illness, Nick Taber asks through his story—arguing that many young people are having valid reactions to environments, while the system recategorizes those reactions as disorders.
With an estimated 21% of kids are diagnosed with a psychiatric disorder, this is a defining management of how children are being taken care of in modern society, Nick first notes.
Yet for many of these children, they are living in families that may be difficult or even abusive. Adults can also be embedded in contexts that feel insufferable. In that case, he said, “for many of us, we’re simply having valid responses to the environments we’re in.”
In a challenging situation like this, someone’s feelings and reactions to an “insufferable situation” too often “get recategorized as a medical problem”—which he says, denies reality and erases what someone is really experiencing.
“I can’t tell you how many people I know who had these mental health services done to them as kids and end up feeling like shells of themselves. And this was certainly my experience for a long time because, and this is the key, we have lost our internal signals that tell us where to go and what to do, that tell us who and what is safe and not safe, what we value in life, what matters, etc.”
6. Don’t guide long-term treatment based on short-term evidence. Anders Sørensen remarks
Anders Sørensen is a clinical psychologist from Denmark who pushes back on the claim that fluoxetine/Prozac can generally be stopped abruptly because of its long half-life. Much of his talk is repeated below:
“In 2018, a study was published in the BMJ asking one very simple question. Do parachutes reduce the risk of death when jumping from an aircraft? The researchers compared two groups, one jumping with and one without. The result, no significant difference between the groups. Parachutes, it seemed, offered no protective effect compared to those jumping without one. But there was one small detail hidden in the method section, which you of course always remember to read. All participants had jumped from an aircraft parked on the ground from an average of half a meter. And as the authors noted, one should be cautious in extrapolating their findings to real world high altitude jumps.
We might laugh at this silly study, but it stops being funny when you realize we’re doing something very similar in psychiatry today. Fast forward to 2025. A study in the American Journal of Medicine compared how long antidepressants were studied in the randomized trials we rely on compared to how long people actually take them.
The median duration of the trials was eight weeks, meaning that most participants had only been on these drugs for two months. And the median duration of real world use in the US, five years.
So we’re using short-term evidence to guide long-term treatment. And that gap matters, especially when it comes to dependence and withdrawal. Time matters because the body adapts.
If you alter brain chemistry for long enough, the body adapts, not overnight, but gradually over weeks and years and months. And the longer that adaptation has been building, the more sensitive it becomes to change and the harder it gets to come off the medication.
In many cases, that can mean tapering over years. Because when you then remove the drug or reduce the dose too quickly, the system is thrown out of balance. And that imbalance is what we call withdrawal. An imbalance between what the system expects and what it now gets at the lower dose.
Since 1997, SSRI withdrawal has been described as mostly mild and self-limiting, lasting a week or two, mentioning only a handful of the more than 80 reported symptoms. That’s what the guidelines say because they’re based on short-term trials far from reality.
So what happens in practice? People who’ve been on these drugs for years, decades, are tapered off as if they’ve been taking them for months. Often by aggressively having the dose, having again stopping. And when that goes wrong, which it often does, they call it a relapse of an underlying condition.”
People come away being told, “well, clearly you still need the medication,” Sørensen explained. So back on the drug people go, with symptoms resolved and an illusion they just learned something fundamentally concerning about their mental health.
Namely: your condition is worse than you think, the medication is demonstrably treating an underlying illness and needs to be part of your long-term experience. Little consideration is given to the possibility that this could simply be withdrawal. Withdrawal has to be ruled out first, before someone resigns to relapse—which can still happen, Sørensen said.
“The trick is to understand withdrawal symptoms for what it is: communication from a body trying to adapt to too big a change too quickly. …What’s confusing is that withdrawal from psychiatric drugs isn’t just physical symptoms. It’s not just dizziness, nausea, headaches, muscle pain, shaking, burning sensations, fatigue. I mean, it’s that too. But it’s also anxiety, insomnia, irritability, depressed mood, mood swings, brain fog, difficulty concentrating, intrusive thoughts.
Withdrawal can mimic relapse or new diagnosis for which there are also drugs. The symptoms overlap. And if you don’t recognize withdrawal, you will misinterpret it.” (This happens in research too, Sørensen explained—with any deterioration often counted as relapse making the drugs look incredibly protective).
If people don’t recognize withdrawal effects, they’ll misinterpret them, Anders explained. “And that’s how people end up on these drugs for years and decades.”
“When stopped, the withdrawal symptoms can be worse than the problems for which the drug was first prescribed,” clinical psychologist Gretchen Lefever Watson likewise said. “Clinicians commonly misinterpret those symptoms as evidence of a worsening condition or the emergence of a new condition.”
“People go in with the side effects and they end up with another… prescription,” Kim Witczak added. “You go in and you’re being told it’s your illness getting worse and there’s no discussion on even how to get off of them.”
Many doctors don’t know about these kinds of dynamics, Sørensen said, because they haven’t been trained to recognize it, let alone how to manage it with proper tapering.
This isn’t about addiction, he explained:
“Just to be clear, this is not about addiction. Antidepressants are not addictive. We’re not talking about cravings or uncontrollable use or people chasing the high.”
What he’s talking about is instead “physical dependence, a state of adaptation manifested by withdrawal syndrome that can be produced by abrupt cessation or rapid dose reduction of the drug. That’s it.”
He described supporting people “through withdrawal reactions from antidepressants so severe you wouldn’t believe they come from a drug, prescribed drug, taken exactly as prescribed. But people aren’t told when they start, they’re not informed. It’s not in the guidelines. So, they find themselves facing unexpected withdrawal, not realizing (it).”
He noted a pattern evident historically:
“This parallels what happened with benzodiazepines introduced first as safe and effective with minimal concern of dependence until decades later, dependence and severe withdrawal became undeniable.”
“Then we saw it again with opioids, again aggressively marketed as safe and effective for chronic pain until we had an epidemic. The pattern is the same.”
“A new drug is introduced, framed as safe and effective, and gets widely prescribed. Then people start having trouble coming off it. Then research begins to confirm what patients are experiencing. But that research is pushed aside, ignored because it challenges the prevailing paradigm.”
“And then the cycle repeats with new safe and effective drugs until we understand this.”
“For context, with benzodiazepines, it took over 40 years from when we knew we had the evidence to when it was formally acknowledged with the blackbox warning in 2020. And if we were to see a similar warning introduced to SSRIs just this year, we’ll only be looking at a delay of around a delay of around 35 years since the first report withdrawal began appearing in the 1990s. And today we’re still drawing conclusions from the ground about what happens.”
7. Secretary Kennedy’s remarks
Anything HHS Secretary Robert F. Kennedy Jr. says gets pilloried and automatically labeled as ridiculous by some people. I think that’s unfortunate, because if there’s one thing Americans across the political spectrum seem to be able to agree with, it’s that our health care system really has some challenges.
This is one of them: a wide onramp onto psychiatric meds, and a very hard to find off-ramp. Feel free to disagree with the Secretary here or on anything else. But as someone who started studying antidepressants almost 25 years ago, I can tell you he is 100% right in what he says in this short talk about mental health and antidepressants:
“The United States does not just face a mental health crisis. We face a dependency crisis driven by overmedicalization. The data is clear. One in six American adults takes an antidepressant. One in 10 children are on prescription medication for their mental health. 30% of college students report using psychiatric medications in the past year.
And in nursing homes, more than half of the residents are on prescribed antidepressants. That’s not a marginal issue. This is a system level pattern. Too many patients begin treatment without a clear understanding of the risks and how long they will stay on these drugs or how to come off of them.
And that’s not informed consent. We are going to fix it.
Today, the Department of Health and Human Services released a dear colleague letter issued by four of my HHS agencies. SAMHSA, CMS, HRSA, and ACF. It directs providers across the country to expand the use of evidence-based nonpharmacologic treatments and to strengthen informed consent and shared decision making.
SAMA, the Substance Abuse and Mental Health Services Administration will publish new data on prescribing trends and release guidance for clinicians and physicians. In June and July, SAMPS will roll out national training modules on psychiatric medication risks on tapering and deprescribing at more than 1,400 federally qualified health centers, community health centers across the country, which treat 39 million patients on how to do medically supervised tapering.
HHS will convene a technical expert panel to develop formal clinical guidelines grounded in evidence and formed by clinicians, patients and their families.
CMS, the Center for Medical, Medicaid, and Medicare Services is issuing billing guidance that allows clinicians to get paid for deprescribing work for the first time. They’ll be paid for care planning, for monitoring withdrawal, for coordinating treatment, and for tracking outcomes.
Psychiatric medications have a role in care, but we will no longer treat them as the default. We will treat them as one option used when appropriate with full transparency and with a clear path off when they are no longer effective.
Patients must understand the benefits, the risks, and the consequences of long-term use before they start, (when) they continue, and when they consider stopping. Without that information, consent does not exist. Right now, gaps in data, labeling, clinical guidance deny patients and physicians the full picture….
We’re also confronting a basic question. What happens when treatment does not work as intended? Some patients report improvement on SSRIs. Others report emotional blunting, loss of motivation, difficulty continuing use, and suicidal ideation.
I watched a family member get off of them after a couple years on them. And she was suicidal literally every day. She woke up every morning and said, “I don’t want to live.” And she said, “The only reason I’m staying alive is for you guys, for the family.” And that’s heartbreaking to hear from a family member. And I’ve heard that from hundreds and hundreds of people. The same story again and again.
(Withdrawal) can be severe. It can be prolonged. And for many patients, it’s completely unexpected.
And the physicians handle this by saying, “Oh, this is your original symptom, reasserting yourself. You need to get back on the SSRIs.”
And they get locked in a lifetime cycle that is uh that for many patients is absolutely cataclysmic. This is a system failure. We’re not going to ignore it.
And let me be clear. If you are taking psychiatric medication, we’re not telling you to stop. We’re making sure that you and your clinician have the information and support to make the right decisions for you. That includes a safe evidence-based path to tapering and discontinuation when clinically appropriate.
At HHS, we are building that path. We are giving clinicians the tools to guide patient safety. We’re giving patients the information to make informed choices because an informed choice is the only choice. Nearly 48 million Americans experienced depression last year. More than 48 million struggled with substance use disorders. These are not abstract numbers.
These are family members. These are individuals. These are people who other people love. That is the scale of the challenge. We are not going to solve it by defaulting to medication. We’re going to solve it by strengthening prevention, expanding non-drug treatment options, and restoring clinical standards that prioritize outcome over volume.